Ozempic, Wegovy, Mounjaro, and Zepbound have become household names fast enough that the pharmacology behind them has struggled to keep pace with the public conversation. Most people know these drugs produce significant weight loss. Far fewer understand the biological mechanism through which they do it, why that mechanism is more sophisticated than simple appetite suppression, or what the current evidence shows about their effects beyond weight and blood sugar. Understanding the biology matters because it changes how patients use the medications, how clinicians prescribe them, and how the broader public evaluates the claims made about them in media that moves faster than the research it is summarizing.
What GLP-1 Is Before It Becomes a Drug
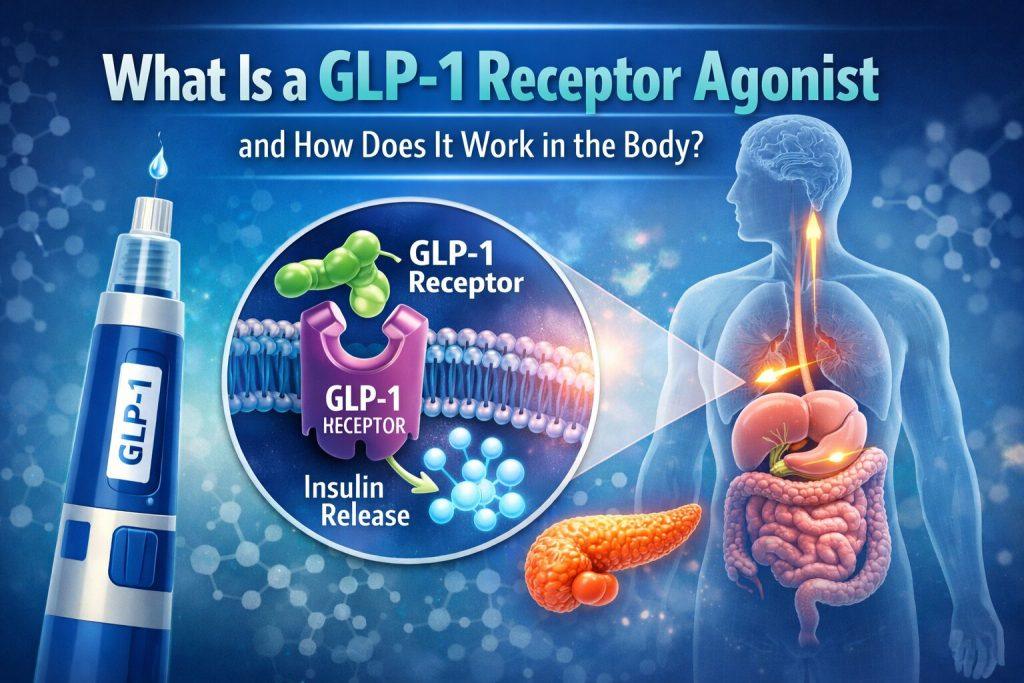
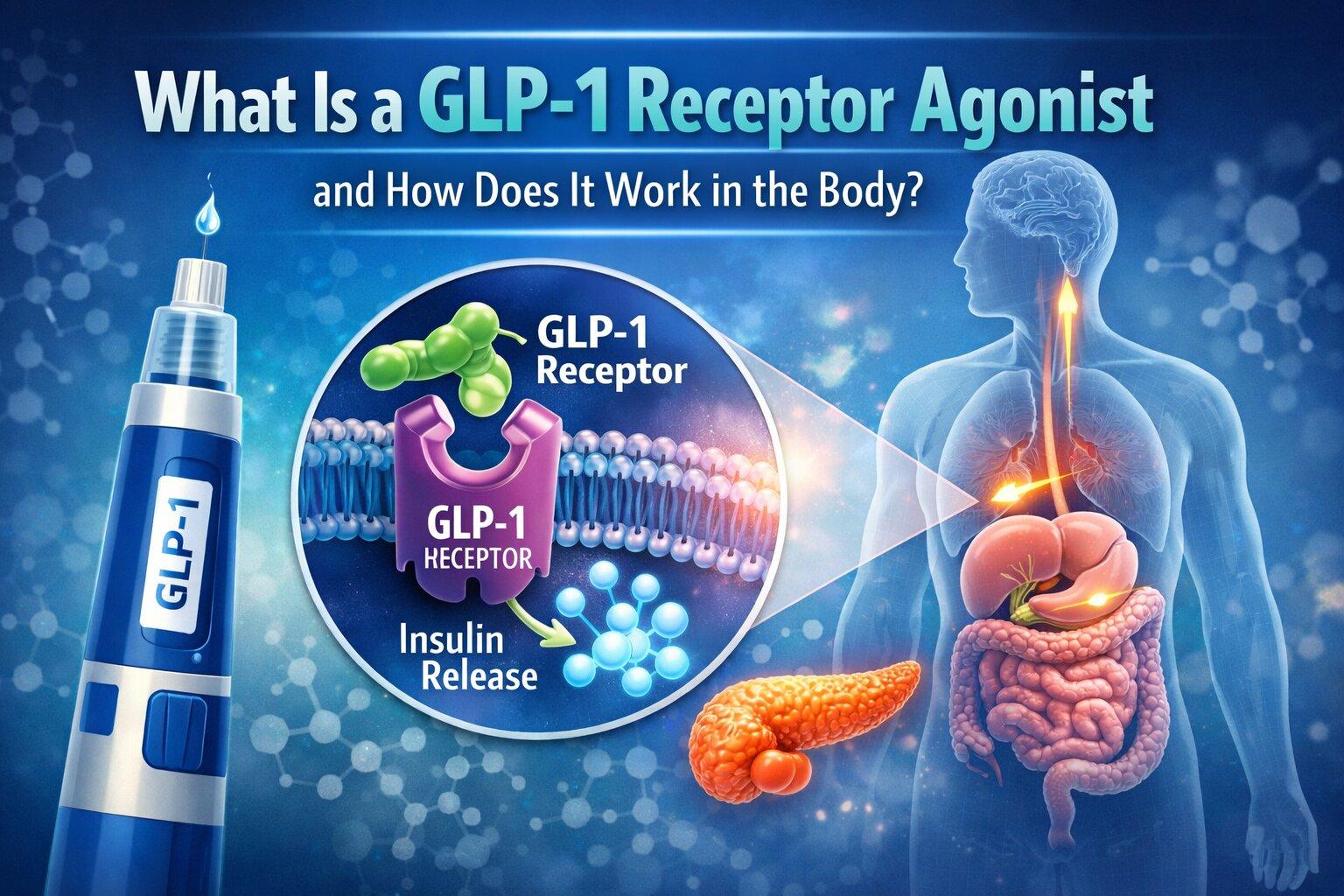
Glucagon-like peptide-1 (GLP-1) is a hormone produced naturally in the L-cells of the small intestine in response to food. When nutrients arrive in the gut after a meal, GLP-1 is released into the bloodstream, where it travels to target tissues including the pancreas, the brain, the heart, the kidneys, and the gastrointestinal tract, binding to GLP-1 receptors on each and initiating a coordinated metabolic response to feeding.
The natural hormone has a critical limitation. Enzymes called dipeptidyl peptidase-4 (DPP-4) degrade it within one to two minutes of release, which means the natural GLP-1 signal is short-lived and produces modest effects compared to what sustained receptor activation achieves. A GLP-1 receptor agonist is a synthetic compound engineered to bind the same receptors as natural GLP-1 but resist DPP-4 degradation, staying active for hours or days and producing a stronger, more sustained version of the same biological signals.
The Four Primary Mechanisms
Research published in the New England Journal of Medicine characterizing the pharmacology of semaglutide and related compounds has identified four primary mechanisms through which GLP-1 receptor agonists produce their clinical effects.
Glucose-dependent insulin stimulation. GLP-1 receptors on pancreatic beta cells respond to activation by releasing insulin, but only when blood glucose is elevated. This glucose-dependency is the feature that distinguishes GLP-1 receptor agonists from older insulin secretagogues, which stimulated insulin release regardless of blood glucose and therefore carried significant hypoglycemia risk. The glucose-dependent mechanism produces effective blood sugar control with a substantially safer side effect profile.
Glucagon suppression. Glucagon, released by pancreatic alpha cells, signals the liver to release stored glucose into the bloodstream. In type 2 diabetes, glucagon secretion is often dysregulated, producing elevated fasting blood glucose even without food intake. GLP-1 receptor activation suppresses glucagon secretion, reducing this excess hepatic glucose output and contributing to improved fasting glycemia alongside the postprandial effects of insulin stimulation.
Gastric emptying delay. GLP-1 receptors in the gastrointestinal tract slow the rate at which the stomach empties its contents into the small intestine. The clinical consequences are a blunted postprandial glucose spike, extended feelings of fullness after eating, and reduced total food intake across the day. This mechanism is also responsible for the most common side effects of the medication class, including nausea, bloating, and early satiety, which are most pronounced during dose escalation and typically reduce as the body adjusts.
Central appetite regulation. GLP-1 receptors are expressed throughout the brain, particularly in the hypothalamus and brainstem regions that regulate hunger, satiety, and food reward. Activation of these receptors reduces the neurological drive toward eating, dampens the rewarding properties of high-calorie foods, and produces the food noise reduction that patients on these medications consistently describe. Research published in Nature Neuroscience has documented that GLP-1 receptor activation in the nucleus accumbens, the brain’s primary reward processing center, reduces dopamine release in response to food cues, providing a neurological mechanism for the reduced food preoccupation and altered food preferences that patients report.
The Drug Classes and Their Differences
Not all GLP-1 receptor agonists are identical, and the differences between them are clinically meaningful.
Semaglutide is the most extensively studied compound in the class. Administered as a once-weekly subcutaneous injection under the brand names Ozempic for type 2 diabetes and Wegovy for obesity management, it has produced average weight loss of approximately 15 percent of body weight over 68 weeks in the STEP-1 trial and demonstrated significant cardiovascular risk reduction in the SELECT trial published in the New England Journal of Medicine in 2023. Oral semaglutide, sold as Rybelsus, is available as a daily tablet with lower and more variable bioavailability than the injectable form.
Tirzepatide, sold as Mounjaro for diabetes and Zepbound for obesity, is a dual agonist that activates both GLP-1 receptors and glucose-dependent insulinotropic polypeptide (GIP) receptors, a second gut hormone involved in insulin secretion and fat storage. Research from the SURMOUNT-1 trial published in the New England Journal of Medicine found that tirzepatide at its highest dose produced average weight loss of 22.5 percent of body weight over 72 weeks, with approximately 37 percent of participants losing more than 25 percent of body weight, outcomes that begin to approach average bariatric surgery results.
Liraglutide, sold as Victoza for diabetes and Saxenda for obesity, is a once-daily injectable that was the first GLP-1 receptor agonist approved specifically for obesity management. It produces smaller average weight loss than semaglutide or tirzepatide and has been partially displaced in clinical practice by the newer once-weekly options, though it remains relevant for patients who do not tolerate semaglutide.
Who Qualifies and Who Does Not
Current FDA approvals for GLP-1 receptor agonists in obesity management apply to adults with a body mass index (BMI) of 30 or above, or adults with a BMI of 27 or above who have at least one weight-related comorbidity including hypertension, type 2 diabetes, or obstructive sleep apnea. For type 2 diabetes management, eligibility is determined by glycemic control targets rather than BMI.
Contraindications include a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 (MEN2), based on findings from rodent studies showing thyroid C-cell tumors at high doses, though a direct causal link in humans has not been established. Prior history of pancreatitis requires careful evaluation, as research published in Diabetes Care has found a small increase in pancreatitis risk associated with GLP-1 receptor agonist use in some analyses.
The Side Effect Profile
Gastrointestinal side effects are the most common and most clinically significant tolerability challenge with GLP-1 receptor agonists. Nausea affects approximately 40 to 50 percent of patients during dose escalation, with vomiting, constipation, and diarrhea also commonly reported. The standard clinical approach is slow dose titration over several weeks to months, which significantly reduces the frequency and severity of gastrointestinal side effects compared to rapid escalation.
Muscle mass loss during weight reduction on these medications has emerged as an important clinical concern. Research published in Diabetes, Obesity and Metabolism found that lean mass constituted a meaningful proportion of total weight lost in patients not receiving specific protein and exercise guidance, with implications for resting metabolic rate, physical function, and long-term weight maintenance. Most prescribing clinicians now recommend protein targets of 1.2 to 1.6 grams per kilogram of body weight daily alongside regular resistance training as companion prescriptions to the medication.
The Cardiovascular and Emerging Evidence
The cardiovascular outcomes data from GLP-1 receptor agonist trials has exceeded expectations in both magnitude and breadth. The SELECT trial demonstrated a 20 percent reduction in major adverse cardiovascular events in people with obesity and established cardiovascular disease but without diabetes, the first time any weight loss medication had demonstrated this benefit in a rigorous outcomes trial in a non-diabetic population.
The FLOW trial of semaglutide published in the New England Journal of Medicine in 2024 demonstrated significant kidney protection in people with type 2 diabetes and chronic kidney disease, reducing the composite risk of kidney failure and cardiovascular death by 24 percent compared to placebo. Trials in heart failure, sleep apnea, alcohol use disorder, and cognitive decline are ongoing and producing early signals that place GLP-1 receptor agonists among the most broadly active drug classes in current clinical investigation.
The GLP-1 vs bariatric surgery data represents one of the most clinically important comparisons in obesity medicine today, as the weight loss outcomes of the newest GLP-1 receptor agonists have closed the gap with average surgical outcomes sufficiently to make the choice between pharmacological and surgical treatment a genuinely complex clinical decision rather than a straightforward preference for the more established and more potent intervention.
Leave a Reply